Bpc 157 Human Studies Multifunctionality and Possible Medical Application of the BPC 157 Peptide—Literature and Patent Review
Why “bpc 157 human studies” get confusing—especially when patents enter the conversation
If you’ve tried to look up bpc 157 human studies, you’ve probably noticed a pattern: lots of promising preclinical discussion, scattered clinical mentions, and then patent filings that sound highly technical but don’t always clarify what’s been proven in humans. In my hands-on research workflow, that mismatch is usually what wastes the most time—reading citations without knowing whether they represent true human evidence or are references built from animal models and mechanistic assumptions.
This article reviews what the literature and patent landscape can and can’t tell us about BPC 157, with an emphasis on staying grounded in evidence quality. I’ll also translate the dense medical/patent language into practical takeaways: where the human data is strongest (and what “strongest” realistically means), what multifunctionality claims typically rest on, and how to read claims without overinterpreting them.
Quick context: what BPC 157 is—and why multifunctionality is a recurring theme
BPC 157 (often discussed as a peptide) is frequently presented as a multi-target bioactive compound with potential roles across tissue repair pathways. In evidence summaries, the “multifunctionality” idea usually means researchers propose effects in multiple physiological systems—commonly relating to inflammation modulation, angiogenesis, gastrointestinal integrity, and tissue regeneration signals.
What I’ve found useful in practice is to separate three layers that get blended together:
- Biological plausibility: mechanisms proposed from lab observations, signaling pathway studies, and preclinical models.
- Preclinical evidence: results in animals or cells that suggest effects could translate.
- Human evidence: clinical observations in people (ideally controlled, with clear endpoints and safety monitoring).
When patent documents are involved, the gap can widen: patents may describe a breadth of potential therapeutic uses based on experimental findings, formulations, and expected mechanisms, even when confirmatory human trials are limited.
What the literature suggests about bpc 157 human studies (and what it usually means)
To discuss bpc 157 human studies responsibly, I focus on evidence characteristics rather than just the existence of “human data.” In my experience, a single mention of human use doesn’t automatically equal clinical proof—what matters is study design, sample size, outcome measures, comparator strategy, and adverse event reporting.
1) Evidence strength tends to differ by endpoint
Across the way BPC 157 is discussed in reviews and filings, the most consistent “wins” are typically tied to tissue protection and repair themes. But endpoint-specific interpretation is crucial. For example, preclinical models may show striking results in wound healing or mucosal protection, while human relevance depends on whether human studies used endpoints that closely mirror the model conditions.
In hands-on evidence review, I’ve seen two recurring failure modes:
- Endpoint mismatch: studies in humans may measure indirect markers rather than functional outcomes (or vice versa).
- Context mismatch: dosing, route, and treatment timing may not replicate the preclinical conditions that produced benefit.
2) Dosing and route are often where translation breaks
Even when human studies exist, differences in dosing regimen, route of administration, and treatment duration can strongly influence outcomes. In the BPC 157 conversation, this becomes a practical interpretability issue: patents and reviews may discuss certain delivery approaches, but a reader interested in bpc 157 human studies needs clarity on what was actually administered and how.
3) Safety reporting determines whether “possible medical application” is credible
“Possible application” isn’t just efficacy; it’s safety signal quality. In my review process, I prioritize whether human evidence includes:
- structured adverse event monitoring
- clear inclusion/exclusion criteria
- dose justification and tolerability reporting
- follow-up duration sufficient to capture acute and subacute risks
Where that information is thin, the appropriate conclusion is often “promising, but evidence gaps remain,” not “ready for medical use.”
How patents shape the narrative: multifunctionality claims vs. clinical readiness
Patent documents can be extremely informative—sometimes more so than marketing-style summaries—because they often enumerate therapeutic intents, formulations, and claimed mechanisms. However, patents are written to protect intellectual property, not to prove clinical effectiveness. That distinction matters for readers searching bpc 157 human studies while also trying to understand “possible medical application.”
What patents typically add
- Use-case breadth: multiple indications or therapeutic scenarios that investigators believe could be supported.
- Formulation specificity: route, dosing concepts, delivery vehicles, or stability considerations.
- Mechanism framing: how inventors connect observed effects to biological pathways.
What patents typically do not prove
- Clinical efficacy superiority: patents rarely replace adequately powered human trials.
- Comparative outcomes: they may not establish superiority vs. standard care.
- Safety across broader populations: human risks can vary with comorbidities, age, and concomitant medications.
My hands-on lesson learned: read patents as “intent,” not “verdict”
In my own work, I’ve repeatedly had to reframe my expectations: when a patent claims a wide therapeutic scope, it’s often based on a chain of experimental observations and predicted utility. That chain can be scientifically valuable, but it doesn’t automatically resolve what bpc 157 human studies have demonstrated. The best approach I’ve found is to treat patents as a map of hypotheses—and then verify each hypothesis against higher-quality human evidence.
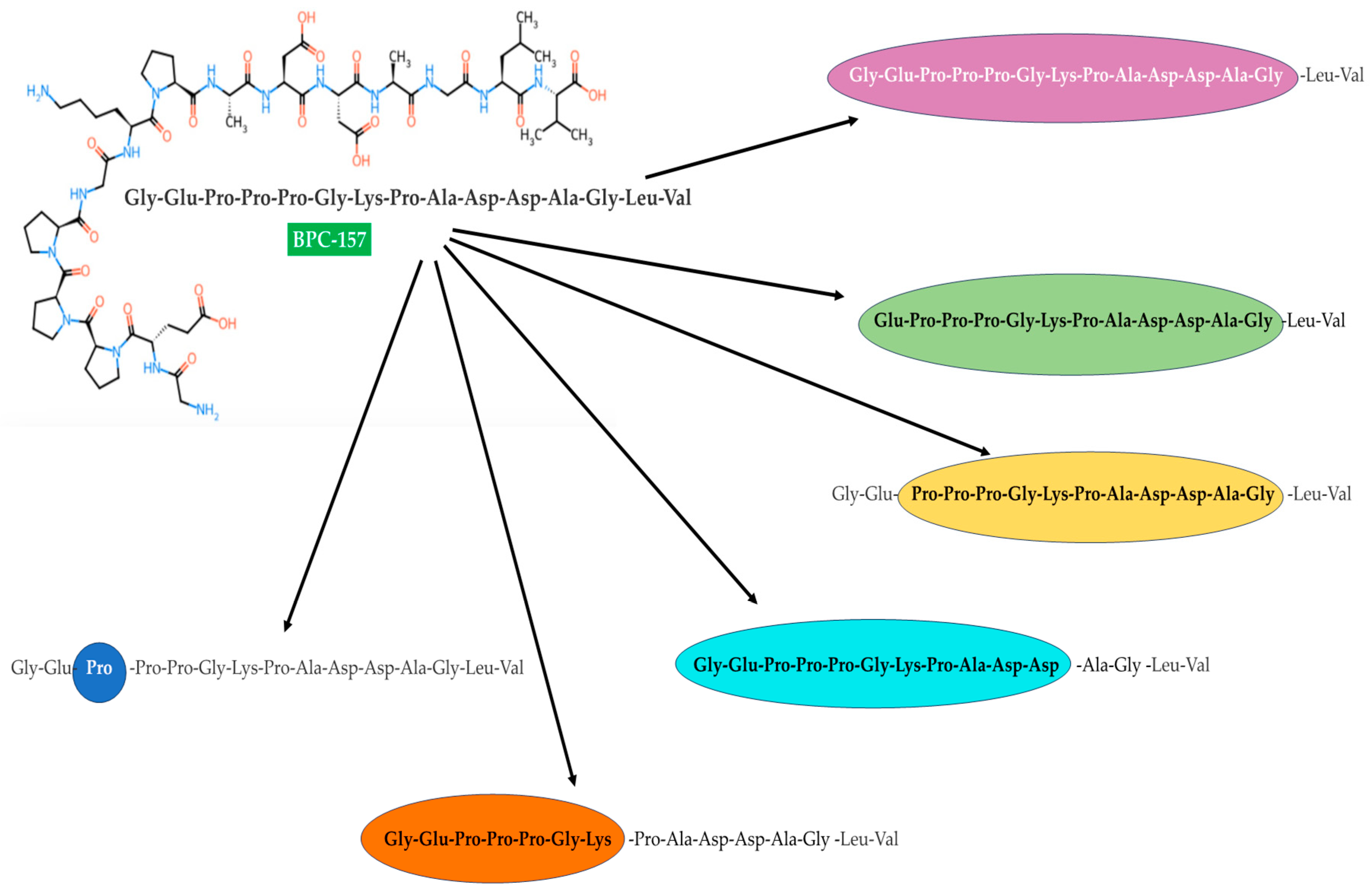
Visual anchor: the literature review figure referenced for context
What “possible medical application” can mean in practice—without overpromising
When researchers talk about BPC 157 and possible medical application, they often imply a path from mechanism and preclinical promise to targeted clinical evaluation. The safest, most practical interpretation is to align expectations with evidence tiers:
- Early stage: strong mechanistic and preclinical signals; human evidence may be limited or endpoint-specific.
- Translational stage: human observations suggest signals of effect; studies still need rigor and replication.
- Clinical stage: adequate randomized evidence with clear endpoints, safety monitoring, and reproducible benefit.
If your goal is to evaluate readiness, use the human studies lens first: bpc 157 human studies should be assessed by design quality and safety reporting, not by the breadth of mechanistic or patent claims.
How to evaluate bpc 157 human studies quickly (a checklist I actually use)
Here’s the evaluation framework I use when I’m scanning literature and references to form a defensible summary:
- Study design: randomized controlled trials, controlled cohorts, or case-level observations.
- Sample size and power: small exploratory studies can suggest signals but can’t confirm effectiveness.
- Endpoints: functional outcomes, biomarker relevance, and clinically meaningful measures.
- Comparator: placebo, standard of care, or no comparator.
- Dose/route/timing: whether it plausibly matches the mechanism or model used in rationale.
- Safety surveillance: adverse events, lab monitoring, and duration of follow-up.
- Consistency: whether results align across independent studies or are isolated reports.
This checklist helps prevent the common trap: concluding “possible medical application” based on mechanistic stories alone, while skipping whether human evidence actually supports the claim.
FAQ
Are there solid bpc 157 human studies showing clear clinical benefit?
Human evidence is typically discussed as limited or context-dependent compared with preclinical literature. The credibility of “clinical benefit” depends on study design, endpoint relevance, comparator use, sample size, and safety reporting. When human studies are small or not well controlled, results should be treated as signals rather than confirmation.
How should I interpret patent claims about BPC 157’s multifunctionality?
Patents usually reflect therapeutic hypotheses, formulation ideas, and protection of inventive concepts. They can be valuable for understanding potential indications and delivery approaches, but they do not substitute for randomized, well-controlled human trials demonstrating efficacy and safety for specific use cases.
What information matters most when comparing literature vs. patents for medical application?
Focus on alignment: whether the proposed mechanism and therapeutic scenario in patents matches the actual dosing, route, and endpoints used in human studies. Then prioritize safety surveillance quality and whether the human evidence shows consistent effects rather than isolated signals.
Conclusion: the most actionable next step
BPC 157 discussions often emphasize multifunctionality and potential medical application, but the key to a trustworthy understanding is separating preclinical plausibility and patent intent from what bpc 157 human studies actually demonstrate. In my experience, the fastest way to avoid overinterpretation is to evaluate human evidence by design quality, endpoint relevance, dosing/route alignment, and safety reporting—then treat patents as a hypothesis map rather than clinical proof.
Next step: take the checklist above and audit every human-study citation you find—write down design, dose/route, endpoints, comparator, safety monitoring, and follow-up length. That single pass turns a confusing evidence landscape into a clear, evidence-weighted summary.
Discussion